


Current design technology and construction methodologies are changing and advancing the way projects are designed and constructed but they are often not aligned with a health systems procurement practices or equipment vendor sales strategies. This disconnect is a complicated chasm to bridge.
The integration of technology and medical equipment into a construction project is critical to its overall success. Managing the integration in a timely manner while mitigating risk and reducing costs is one of the main responsibilities for the healthcare project manager. Aligning independent divergent processes are critical for superior project outcomes.
CHANGING THE DECISION MAKING CYCLE
Within a healthcare project, the furniture, fixtures, and equipment (FF&E) and medical equipment can constitute between 20%-40% of the overall budget. Procuring furniture and equipment requires detailed attention in the specification and ordering process to ensure the most competitive price, latest technology and fastest speed to market. Early revenue generation and return on investment (ROI) drive the majority of decisions regarding the medical equipment selection. The challenge facing healthcare organizations is how to change their decision making procurement cycle to best meet the new design paradigm created with the construction industry.
Within the last seven years, there has been a shift in how the design industry conducts schematic and design development meetings and the information they require to be efficient. Building information modeling (BIM) requires more upfront direction and decision making earlier in the process to allow for the models to be built. In the past, these decisions and their coordination efforts were made later during the design development or construction documentation phase.
BIM has been a huge asset in resolving clash detection and design conflict issues prior to construction. It also allows for pre-construction of materials delivered to the site, which increases quality and decreases schedule durations. BIM coordination has dramatically reduced change orders during the construction period, but, unfortunately, it has had the opposite effect on medical technology integration. BIM requires that medical equipment decisions be made earlier. The dichotomy of the health system’s vendor selection process versus the equipment vendors business model results in excessive change orders on projects.
"BIM requires that medical equipment decisions be made earlier. The dichotomy of the health system’s vendor selection process versus the equipment vendors business model results in excessive change orders on projects." — Julie Ford, CBRE Healthcare
PROCUREMENT STRATEGY REALIGNMENT
Equipment vendors will not do site specific drawings for large fixed equipment, such as MRIs, X-rays, and CTs, until they have an order and purchase order number in hand. Once the BIM drawings are complete, there will usually be changes that are required for power/data locations, HVAC requirements, and even millwork to accommodate the equipment in the room. When these changes occur during construction it has a major negative effect on the project budget and schedule. Getting all of the players to the table early to make equipment decisions prior to construction will save significant time and money. This obvious solution rarely occurs.
In discussions with procurement specialists, bio-med specialists, information systems analysts, and medical equipment vendors, everyone agrees that there is a problem, but few offer a solution. Including all team members early, communicating often, and setting realistic budgets is only part of the answer.
PROPER COMMUNICATION LEADS TO POSITIVE RESULTS
Successful projects require positive and constant communication among all team members. Including stakeholders that are not traditionally engaged at the beginning of a project creates an environment for productive communication and also:
1. Provides knowledge and buy-in from stakeholders and allows for a clearer understanding of design decisions, project definitions, and “lines in the sand” related to project changes.
2. Brings a different perspective to the project and opens dialogue that the design team, construction team, or project manager may not be aware of regarding equipment limitations and future technologies that need to be planned for or corporate standards that user groups may not be aware of.
3. Changes the procurement timeline so supply chain can negotiate equipment further in advance of when it is needed resulting in potential cost savings, early production of site specific drawings, and better construction coordination.
EQUIPMENT UPGRADES AND ENHANCEMENTS
Changing advancements in healthcare is a significant project challenge. Healthcare organizations often submit POs for large equipment one to two years in advance of delivery to secure the best pricing. Contracts typically state that the client will receive the latest technology available at the time of delivery. If the new equipment varies in size, power/data or technological enhancements this could cause cost and schedule issues for the project. Upgrades/alterations result in last minute change orders that may be very costly. Unfortunately, vendors often have non-disclosure agreements that prohibit them from sharing new technology upgrades, even with a PO in place.
At a large ambulatory surgery center with four OR’s, 16 pre/post-op bays, minor procedure rooms, and four GI/Endo rooms, the team specified a monitor and bracket to hang on the head wall in the pre/post-op bays and on the booms in the ORs and procedure rooms. The original equipment order was placed in December 2013 as part of a larger order, securing deep discounted pricing. Receipt of the equipment will be in spring 2015.
The current specified monitor, which required one data drop, has now been discontinued. The vendor will still warranty the item and maintain parts for five years, but the hospital would be basically purchasing new equipment that has reached obsolescence. These types of purchases typically occur every 15 to 20 years, and not in the best interest of the client. As per the contract, the upgraded unit they would receive required two data drops.
If the design team had been aware of this new feature during the BIM design or the beginning of BIM construction, the power/data requirements could have been added with little or no cost impact to the project. Instead, installing 45 additional data drops a few months prior to completion had a significant impact on the project. The actual cost of adding 45 data drops to the project in labor and materials was expensive. The contractor had to return to spaces previously completed to make the changes.
In the end, the change order totaled over $80,000. This seemingly minor port change to the vendor equipment had significant implications to the overall project budget and schedule. If the equipment vendor could have alerted the client to the design/feature changes earlier this could have been avoided.
There are two solutions to address this issue. As previously mentioned, the project manager’s role is to mitigate risk and cost. In addition, they must foster a culture of participation and trust between the equipment vendor and the health system’s procurement department.
One of the largest obstacles is the proprietary nature of technological advances and product enhancements to the medical equipment. Vendors are hesitant to discuss changes and upgrades prior to product release. This is contradictory to a collaborative customer/vendor relationship. If an equipment vendor has a health system’s PO (which is an expression of trust between the supplier and the client) and the client agrees to sign a NDA, the vendor should be able to review items ordered and advise the client of upcoming changes as soon as possible.
The way to mitigate change orders related to medical equipment is to have the HVAC/electrical/data requirements examined, planned for and reviewed early in the process by the vendor, prior to construction. This is the disconnect between the vendor’s sales strategy and the client’s procurement strategy. Navigating solutions and negotiating terms prior to order entry can reduce risk and cost. Another recommendation is for the project manager to alert the client to any potential issues and if warranted, advocate for an equipment contingency within the total project budget to cover change orders beyond typical construction contingencies.
CONCLUSION
Fixing project disconnects that can derail a facility project related to medical equipment integration can be overcome by involving procurement, FMS, IS, and bio-med specialists at the beginning of a project. In addition, early vendor integration, good project communication and appropriate budget allocation will align the appropriate strategies of all stakeholders. This will not occur on its own. It is dependent upon the direction and guidance of a strategic minded project manager. Fostering a collaborative environment that is focused on the overall project, as opposed to individual outcomes and divergent business models, will best position your next healthcare project to handle the ever changing evolving technology landscape and ensure success.
About the Author: Julie Ford is the Director of Healthcare Project Management at CBRE Healthcare.
Related Stories

| Sep 19, 2013
Roof renovation tips: Making the choice between overlayment and tear-off
When embarking upon a roofing renovation project, one of the first decisions for the Building Team is whether to tear off and replace the existing roof or to overlay the new roof right on top of the old one. Roofing experts offer guidance on making this assessment.

| Sep 17, 2013
Healthcare project will merge outpatient clinic with YMCA to promote wellness and prevention
Penrose-St. Francis Health Services and the YMCA of the Pikes Peak Region announce collaboration, along with developer The Boldt Company, to create next-generation wellness facility.

| Sep 16, 2013
Study analyzes effectiveness of reflective ceilings
Engineers at Brinjac quantify the illuminance and energy consumption levels achieved by increasing the ceiling’s light reflectance.

| Sep 11, 2013
BUILDINGChicago eShow Daily – Day 3 coverage
Day 3 coverage of the BUILDINGChicago/Greening the Heartland conference and expo, taking place this week at the Holiday Inn Chicago Mart Plaza.

| Sep 10, 2013
The new medical office building: 7 things to know about today’s outpatient clinic
Regulatory pressures, economic constraints, and emerging technologies are transforming healthcare. Learn how Building Teams are responding with efficient, appealing, boundary-blurring outpatient buildings.

| Sep 10, 2013
BUILDINGChicago eShow Daily – Day 2 coverage
The BD+C editorial team brings you this real-time coverage of day 2 of the BUILDINGChicago/Greening the Heartland conference and expo taking place this week at the Holiday Inn Chicago Mart Plaza.

| Sep 4, 2013
Augmented reality goes mainstream: 12 applications for design and construction firms
Thanks to inexpensive mobile devices and increasingly advanced software apps, Building Teams are finally able to bring their BIM models to life on the job site.
| Sep 4, 2013
Smart building technology: Talking results at the BUILDINGChicago/ Greening the Heartland show
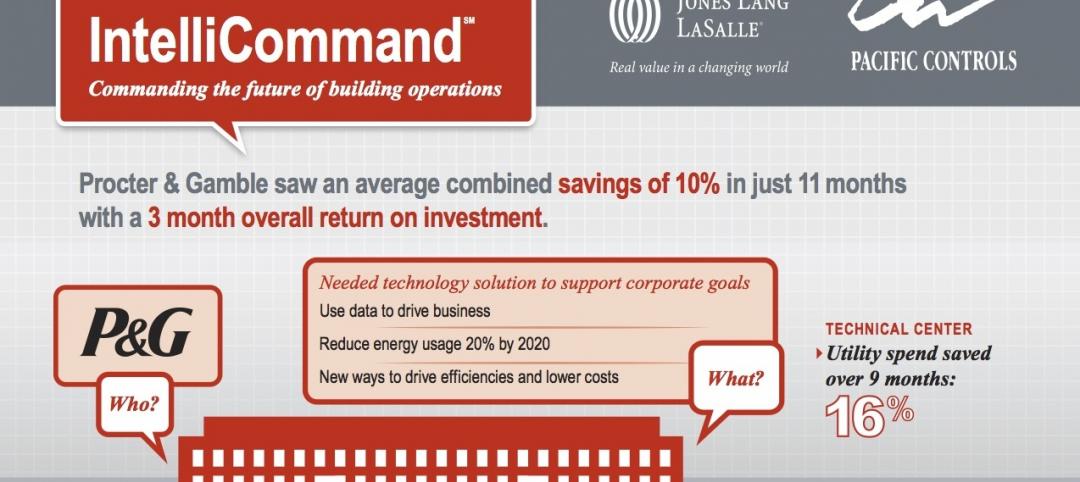
Recent advancements in technology are allowing owners to connect with facilities as never before, leveraging existing automation systems to achieve cost-effective energy improvements. This BUILDINGChicago presentation will feature Procter & Gamble’s smart building management program.

| Aug 30, 2013
A new approach to post-occupancy evaluations
As a growing number of healthcare institutions become more customer-focused, post-occupancy evaluations (POE) are playing a bigger role in new construction and renovation projects. Advocate Health Care is among the healthcare organizations to institute a detailed post-occupancy assessment process for its projects.

| Aug 26, 2013
What you missed last week: Architecture billings up again; record year for hotel renovations; nation's most expensive real estate markets
BD+C's roundup of the top construction market news for the week of August 18 includes the latest architecture billings index from AIA and a BOMA study on the nation's most and least expensive commercial real estate markets.



