


A lot can happen and change in five years, and a lot has in healthcare. But to some degree many things have stayed the same due to resistance, being ignored, or just slow to change.
It has been five years since the Patient Protection and Affordable Care Act (PPACA, or ACA for short) was signed into law in March of 2010. Since that time, we have seen a continued shift to outpatient care, high utilization of hospital-based and free-standing emergency departments, the evolution of public and private insurance exchanges, the beginnings of defining quality and service metrics, and a slow migration from volume-based “first curve” world toward a value-based “second curve” industry.
The smart money is on shifting toward lower-cost, high-value care wrapped by a population health management mentality. Even if the payer system never moves fully to value-based, the more efficient and efficacious health systems emerging from this migration will be well positioned to provide competitive, low cost care in a volume-based or value-based system.
WHAT DO THE STATISTICS SAY?
An intended outcome of the ACA and reform is to reduce overall inpatient activity by managing health, reducing average length of stay (ALOS), reducing readmissions, and generally moving toward a holistic approach of population health rather than an acute, episodic approach.
Many are still skeptical that change is possible and that the government-sponsored system will fail. But data from the American Hospital Association (AHA) shows some interesting trends. From 2010–2012 (2012 is the latest data available at a national level), overall patient days and patient days per 1,000 population have declined. The number of inpatient beds has stabilized and decreased slightly, while emergency department visits and hospital-based outpatient visits continue to increase.
For years, pundits have postulated that with population increase and the aging Baby Boomer impact, inpatient utilization would increase. But what has happened overall, and in most markets, is the opposite. Inpatient days are declining.
In a Midwest market where CBRE Healthcare is currently working, Truven Health Analytics is projecting an overall inpatient use rate decline over the next five years. In many markets, providers are turning to Milliman models (Truven and Milliman provide data and consultative services to the healthcare industry related to retrospective and prospective healthcare utilization), projecting the impact of managed markets.
Clinical integration continues to increase with more than 60% of community hospitals (non-government facilities) affiliated in some manner with larger integrated delivery systems. Providers are realizing that there is value in integration, including payer leverage, rational distribution of services, access to clinical protocols, access to capital, sharing of clinical information, geographic diversity to better manage population health, and cost distribution to lower the overall cost of care.
Many systems that took part in the Accountable Care Organization pioneer projects have since left them, yet they still continue to develop their own efficient networks of care, partner with providers and payers, partner with community entities, and develop robust primary care networks through either traditional means or the establishment of primary care medical homes.
Regardless of what the government is doing or not doing, the market has responded and is getting ready for a value-based world where the inpatient hospital is no longer the center of the healthcare universe. Will there still be a need for acute-care hospitals? I say, without a doubt, yes.
But our focus on the “hospital on the hill” as the sole location for all of our healthcare needs has changed, and will continue to evolve.
WHAT ARE HEALTHCARE ORGANIZATIONS DOING ABOUT IT?
A sound planning approach that is implementation oriented is required. Time and dollars are too important to leave to hope and chance. The decisions are multi-variate and require a focus on strategy, facilities, real estate, financials, and overall care model.
1. Market Analysis Scenario Planning
A rigorous market analysis focusing on inpatient use rates, market share, and length of stay is required. As inpatient discharge rates decrease, so will overall bed demand.
This is an intended consequence of the ACA and the move to a value-based world. The goal is to manage hospitals stays (and the high costs associated with these stays) by better managing health.
We are modeling bed demand with several healthcare providers. These models are based on use rates remaining static or dropping, certainly not increasing. In the same models, we are adjusting market share to account for these drops.
But there has to be a corresponding strategy to increase market share, whether it be physician recruitment and alignment or through increased partnerships with other regional hospitals and providers that are referral sources.
Hope is not a strategy, but planning on how to shore up declining inpatient volumes is. As lengths of stay change, efficiency in operations will also demand that ALOS stabilize. All of this points to a steady state or decline in inpatient bed need.
2. Plan for Right-Sizing Inpatient Care
Inpatient care is not going away. However, our nation’s hospitals continue to age and are rife with infrastructure, standard-of-care, and operational issues. In short, they are out of date with contemporary and efficient care delivery.
Investment in inpatient core assets has slowed, and providers struggle with spending dollars when there is no guarantee on return on investment. Having a long-view to provide more efficient “outpatient like” hospitals must be the focus. Downsizing is a reality and re-investing in new/renovated modern facilities is occurring.
3. Plan for Ambulatory Care Strategies
As care continues to shift to ambulatory environments in primary and specialty care, healthcare organizations are seeking strategies and tactics to increase their capture rate of this market. Healthcare systems are developing robust primary care strategies to “blanket” their service area and cover lives.
Providers are also continuing to move “pure” ambulatory functions out of the high-cost, difficult to access, core hospital campus into dedicated, patient and provider friendly ambulatory care centers (ACCs). These ACCs are either on or off the medical campus. If they are on-campus, they should be separate and distinct from the inpatient chassis.
Owners, planners, project managers, architects, and builders need to provide the same level of creativity in site, facilities, and operational planning for ambulatory care as they have done for inpatient care over the last two decades.
CONCLUSION
Ultimately, healthcare providers are seeking direction on how to plan for a value-based world while still very much operating in a volume-based market. Successful organizations will position themselves to cover more lives and establish long-lasting relationships with physicians and other providers while re-tooling their inpatient and outpatient portfolio of assets to meet the changing needs and evolving requirements of payers and consumers.
By improving efficiency and developing broader networks, providers will succeed in today’s market. Following this approach will enhance volume in the short-term while preparing for long-term value-based incentives.
About the Author: Curtis Skolnick is Managing Director with CBRE Healthcare, based in Richmond, Va.
Related Stories

| Nov 19, 2013
Pediatric design in an adult hospital setting
Freestanding pediatric facilities have operational and physical characteristics that differ from those of adult facilities.

| Nov 19, 2013
Top 10 green building products for 2014
Assa Abloy's power-over-ethernet access-control locks and Schüco's retrofit façade system are among the products to make BuildingGreen Inc.'s annual Top-10 Green Building Products list.

| Nov 18, 2013
6 checkpoints when designing a pediatric healthcare unit
As more time and money is devoted to neonatal and pediatric research, evidence-based design is playing an increasingly crucial role in the development of healthcare facilities for children. Here are six important factors AEC firms should consider when designing pediatric healthcare facilities.

| Nov 15, 2013
Greenbuild 2013 Report - BD+C Exclusive
The BD+C editorial team brings you this special report on the latest green building trends across nine key market sectors.

| Nov 15, 2013
Pedia-Pod: A state-of-the-art pediatric building module
This demonstration pediatric treatment building module is “kid-friendly,” offering a unique and cheerful environment where a child can feel most comfortable.

| Nov 14, 2013
Behind the build: BD+C's 'Pedia-Pod' modular pediatric patient unit at Greenbuild 2013 [slideshow]
Next week at Greenbuild, BD+C will unveil its demonstration pediatric patient unit, called Pedia-Pod. Here's a behind-the-scenes look at the construction of this unique modular structure.
| Nov 13, 2013
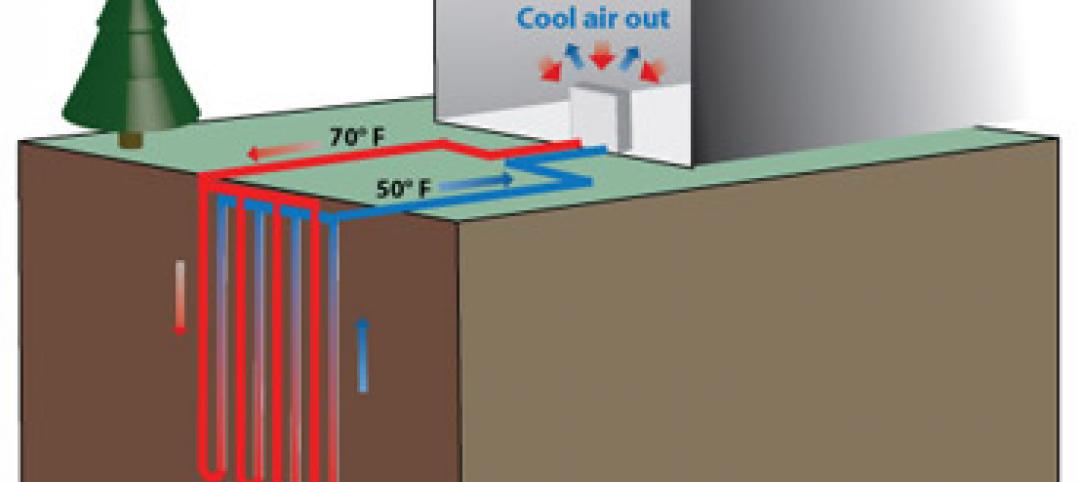
Installed capacity of geothermal heat pumps to grow by 150% by 2020, says study
The worldwide installed capacity of GHP systems will reach 127.4 gigawatts-thermal over the next seven years, growth of nearly 150%, according to a recent report from Navigant Research.

| Nov 8, 2013
Oversized healthcare: How did we get here and how do we right-size?
Healthcare facilities, especially our nation's hospitals, have steadily become larger over the past couple of decades. The growth has occurred despite stabilization, and in some markets, a decline in inpatient utilization.

| Nov 1, 2013
CBRE Group enhances healthcare platform with acquisition of KLMK Group
CBRE Group, Inc. (NYSE:CBG) today announced that it has acquired KLMK Group, a leading provider of facility consulting, project advisory and facility activation solutions to the healthcare industry.

| Oct 30, 2013
15 stellar historic preservation, adaptive reuse, and renovation projects
The winners of the 2013 Reconstruction Awards showcase the best work of distinguished Building Teams, encompassing historic preservation, adaptive reuse, and renovations and additions.



