


Looking at trends and predictions from the beginning of 2013, many anticipated that it would be a transformational year as healthcare organizations evolved to confront the challenges of a changing marketplace. As the year draws to a close and we look to the future, despite the lack of clarity regarding many elements of healthcare reform, there are several core tenets that will likely continue to drive transition within our industry.
While each of these trends is widely acknowledged and publicized, their pervasive impact on healthcare real estate warrants further examination. Healthcare providers will be challenged to provide higher quality care to an expanded patient base at a significantly lower overall cost. To achieve these objectives and thrive in the marketplace of the future, many healthcare organizations will be required to transition and transform their portfolio of real estate assets, as well as the manner in which those assets are planned, financed, constructed and managed.
1. INSURANCE EXPANSION AND REFORM
Expanded Coverage for All?
Until very recently, prevailing expectations held that the Affordable Care Act would result in a net increase in the number of insured Americans by as many as 30 million individuals. However, the highly publicized shortcomings of government sponsored insurance enrollment portals, the relative lack of interest in enrollment among younger age cohorts and the increasing number of individuals receiving coverage cancellation notices in the past two months may actually result in a short term decrease in the total insured population.
Financial Incentives - Focus on Patient Outcomes
Providers have traditionally been compensated for episodes of care. There has been little financial incentive to coordinate care between physicians and many procedures are criticized as contributing little to patient outcomes. This reimbursement environment is commonly criticized as a primary driver in the escalation of healthcare expenditures in this nation.
A central objective of the Affordable Care Act is to transition to a Value Based Reimbursement environment in which “bundled payments” are made to coordinated teams of care providers and are based on patient outcomes rather than the number of procedures performed. There will be little to no reimbursement for patient readmissions. This seismic shift will mandate that high quality patient outcomes are achieved consistently in the most coordinated and efficient manner possible.
Responding to Insurance Expansion and Reform – The Role of Healthcare Real Estate: So, how does real estate enter the discussion regarding insurance and financial incentives? To achieve the objective of delivering best in class patient outcomes in a consistent manner at the lowest possible cost, providers will benefit significantly from standardizing best practices across their organizations. As “form follows function”, healthcare real estate portfolios must be comprised of replicable care environments. It is difficult to expect consistent patient outcomes unless the very environment in which that care is delivered is also consistent.
2. TRANSFORMING THE ORGANIZATIONAL MODEL OF CARE
Here Today....There Tomorrow
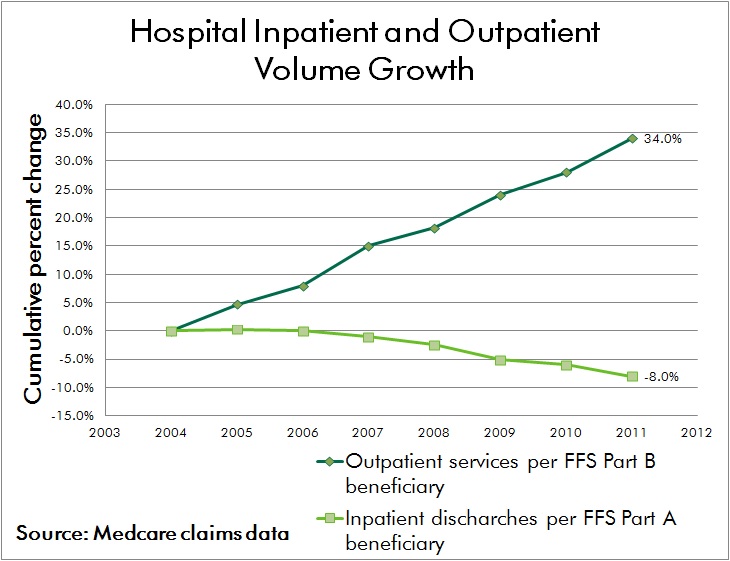
Advances in medical technology have driven a shift in procedural volume to the outpatient environment for decades. With the added imperative to provide care in the lowest cost responsible setting, this trend is expected to continue. Advances in technology will not only enable a continued shift from inpatient to outpatient procedures, but it’s highly likely that certain elements of care currently provided in outpatient and medical office environments can be achieved through remote monitoring and electronic communication while patients remain at home or work.
Organizing for Success
While the physical environment of care continues to shift, the organizational structure of healthcare providers must keep pace as well. The hospital centric model of the past has already given way to a hub and spoke network of care in most markets, where outpatient centers provide convenient and accessible care to patients and refer volumes to affiliated inpatient facilities.
The prevailing hub and spoke network will give way to a distributed model of care that is physically dispersed yet highly integrated. Electronic medical records and advances in medical information technology will allow seamless handoffs between care providers, many of whom will be geographically dispersed across the network. Primary care and internal medicine specialists will coordinate care regimens, a patient centric concept known as the “medical home.”
Responding to Organizational Transformation – The Role of Healthcare Real Estate: Reflecting the significant capital investment in acute care facilities and traditional medical office environments that currently resides on providers’ balance sheets, the transition of healthcare real estate portfolios to nimble, distributed networks of care will be a long term process. Given the lengthy cycle of major facility planning and development schedules, it's imperative that providers initiate coordinated market and facility planning efforts today in order to begin their journey of transformation.
3. MARGIN COMPRESSION
The Future Ain’t What it Used to Be
The seismic shifts in healthcare finance being driven by insurance reform threaten the long term viability of many healthcare providers who have traditionally operated near breakeven. According to Moody's Investors Service, nonprofit hospitals had a strong balance sheer in fiscal year 2012 but profitability metrics were down compared with FY 2011. For the first time since FY 2008, Moody's found that growth in expenses outpaced revenue growth in nonprofit hospitals and health systems. Even a modest shift in revenue outlook for these organizations may constitute the difference between operating in the black or confronting financial loss.
While a substantial portion of the nation’s hospitals and health systems are non-profit institutions, there is common recognition that erosion of financial performance will compromise the ability to provide philanthropic and charity care. “No margin – No mission.” Few expect brighter prospects for revenue; therefore, organizational survival will depend on the ability to decrease expenditures without compromising care.
Competing Demands for Scarce Capital
Despite concern regarding future operating margins, the demand for capital investment is greater than ever. Conversion to electronic medical records is an enormously expensive undertaking, often running into the hundreds of millions of dollars for large health systems. Mergers, acquisitions and affiliations among providers also demand organizational focus and capital.
Responding to Margin Compression – The Role of Healthcare Real Estate: Real estate assets often constitute the single greatest balance sheet asset for healthcare providers and real estate related expenses are typically exceeded only by the cost of labor on providers’ income statements. To meet the imperative of cost reduction, in the most general terms, healthcare real estate must be developed and operated in a more cost effective manner. Facility layouts also have an integral impact on the efficiency of patient care delivery processes; and therefore play a key role in reducing labor expense without compromising quality of care.
4. INDUSTRY CONSOLIDATION
One of the most significant byproducts of insurance reform and financial pressures faced by healthcare providers has been an unprecedented wave of industry consolidation. Many independent hospitals and small health systems are not sufficiently capitalized to effectively reinvest and reinvent themselves. Similar challenges are faced by physicians operating in small group practices as they struggle to cover traditional costs such as malpractice insurance, as well as the added burden of conversion to electronic medical records.
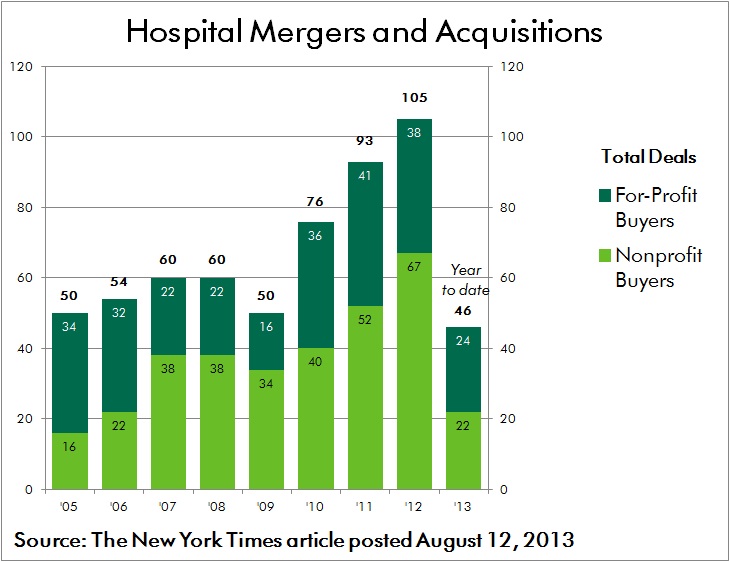
Coupled with the prospect of “bundled payment” reimbursements, these forces are driving consolidation in order to allow providers to better coordinate care and to spread costly investments across a larger operating platform. According to an Irving Levin report, healthcare mergers and acquisitions activity during the third quarter this year soared 16 percent over the second quarter of 2013. There were 267 deals announced, which is 20 percent more than the third quarter last year. Many of these alliances break from the traditional mold, including the acquisition of physician practices by insurance providers.
Responding to Consolidation – The Role of Healthcare Real Estate: As health systems, hospitals and physician groups merge and affiliate, the resulting portfolio of assets is often poorly positioned to serve the organization’s needs in an efficient manner. Fragmented networks of leased and owned facilities are located in close proximity to each other. Multiple systems and protocols are used to manage the development and operation of assets. Legacy policies and procedures are not synchronized.
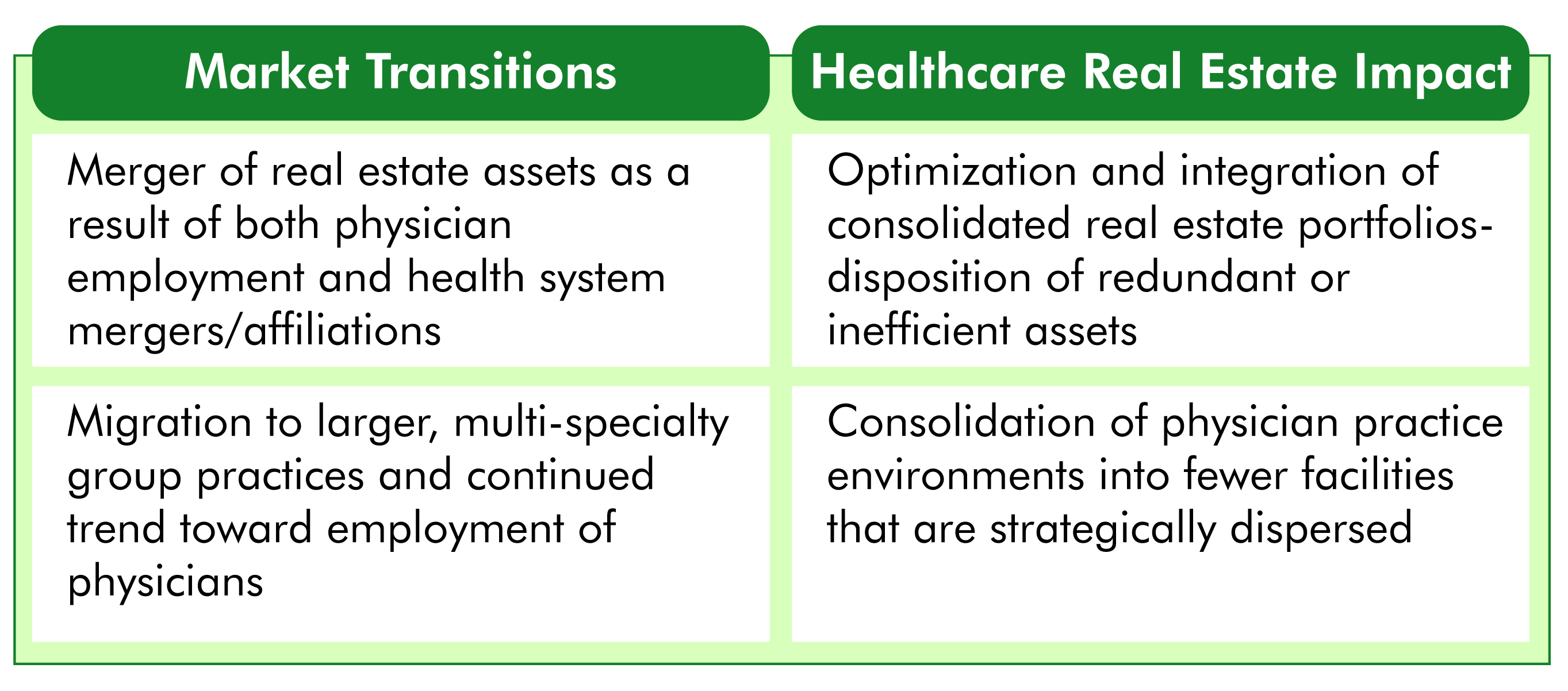
To meet the challenges of coordinated care and cost reduction, a transition plan must be enacted through which optimal facility network distribution and co-location of care providers is achieved. In many cases this will result in the consolidation of redundant and inefficient facilities, while in other cases there will be a need to develop facilities in new markets in order to effectively achieve population health management goals. Migrating to a common, best in class platform for managing consolidated portfolios of facilities often requires investment in both training and new technology.
CONCLUSION
As the pace of transformative change within the industry accelerates, healthcare leaders must heed the call to act decisively in order to position their organizations for survival and success. Effective planning, development and operation of healthcare real estate assets will be a critical element in ensuring that best in class, patient centered care is delivered consistently and cost effectively. As margins are compressed and care is increasingly distributed across broader provider networks, the integration of strategic, financial and facility initiatives is more critical than ever.
Within every challenge lies opportunity. Best wishes to all in capitalizing on those opportunities in the year ahead.
Related Stories
| Feb 13, 2012
New medical city unveiled in Abu Dhabi
SOM’s design for the 838-bed, three-million-square foot complex creates a new standard for medical care in the region.

| Feb 10, 2012
Task force addresses questions regarding visually graded Southern Pine lumber
Answers address transition issues, how to obtain similar load-carrying capabilities, and why only some grades and sizes are affected at this time.

| Feb 10, 2012
Atlanta Housing Authority taps Johnson Controls to improve public housing efficiency
Energy-efficiency program to improve 13 senior residential care facilities and save nearly $18 million.

| Feb 10, 2012
Besculides joins New York Office of Perkins Eastman as associate principal
Besculides joins with more than 17 years’ experience in design, business development, and account management for the government, healthcare, and corporate practice areas with a particular focus on the financial and media sectors.

| Feb 10, 2012
Mortenson Construction research identifies healthcare industry and facility design trends
The 2012 Mortenson Construction Healthcare Industry Study includes insights and perspectives regarding government program concerns, the importance of lean operations, flexible facility design, project delivery trends, improving patient experience, and evidence-based design.

| Feb 10, 2012
LAX Central Utility Plant project tops out
Construction workers placed the final structural steel beam atop the Plant, which was designed with strict seismic criteria to help protect the facility and airport utilities during an earthquake.

| Feb 8, 2012
Nauset completes addition and renovation for Winchester senior living community
Theater, library, fitness center, and bistro enhance facility.

| Feb 8, 2012
Mega-malls expanding internationally
Historically, malls have always been the icons of America – the first mall ever was built in Minneapolis in 1956.

| Feb 8, 2012
World’s tallest solar PV-installation
The solar array is at the elevation of 737 feet, making the building the tallest in the world with a solar PV-installation on its roof.

| Feb 7, 2012
AIA introduces seven new contract documents to Documents-On-Demand service??
AIA Contract Documents are widely-used standard form contracts among the building industry to support construction and design projects.



