

Many healthcare institutions have invested considerable time re-thinking the use of clinical space to increase capacity for COVID-19 patients. Could this experience be leveraged and scaled to meet a future surge—driven by a pandemic or other extreme emergency events—if considered proactively and at a larger, district scale?
The current COVID-19 pandemic highlights the concern that we will see more emergency events in the coming years. Future incidents may include epidemics, pandemics, natural disasters and large-scale terrorist attacks. One opportunity to develop greater resiliency to these events may be a reconsideration of the inter-institutional planning at the medical district level.
Many medical districts are urban developments that co-located healthcare providers and allied organizations, usually centered on a major academic medical center and often spread over several city blocks. Medical districts and communities increasingly encompass clinical providers, health educators, biomedical research, insurance and manufacturing, supported by commercial business, residential, retail and transportation hubs in one large urban district specifically zoned to attract and support health industries.
Significant healthcare capacity resides in these medical districts and academic medical centers. Harnessing these capabilities could optimize the proximal resources of multiple institutions to meet a diverse range of emergent population needs, such as treatment spaces, lab space for testing and development of therapeutics, housing for providers, and conference space for communications and command/control.
Optimizing Resources and Capacity
The diversity and capacity of resources in a medical district are substantial. For example, Boston's Longwood Medical Area (LMA) has grown organically around Harvard Medical School and includes Beth Israel Deaconess Hospital, Brigham & Women's Hospital, Boston Children's Hospital, Dana-Farber Cancer Institute and Joslin Diabetes Center—all located within a quarter-mile radius of each other. These five institutions have approximately 1,900 inpatient beds and over 24 million square feet of space. If the adjacent colleges are included, the number of physical beds in the LMA increase to almost 9,000. Factor in the hospitals' emergency departments, perioperative bays, treatment areas and exam rooms—most of them connected by bridges and tunnels—and there is the potential for create a super-resource to address the needs of a future emergency event.
Other examples abound across the country and include Anschutz Medical District in Denver, UCSF Mission Bay Medical Center in San Francisco, Texas Medical District in Houston and the UIC Medical District in Chicago.
Under emergency conditions, each hospital in a district may individually take steps to increase treatment capacity. However, the ability to effectively meet surge demand may depend on these ease with which patients, staff and materials can be physically and operationally distributed across the medical district, enabling a nimbler response to the changing and unpredictable conditions. The ability to effectively aggregate resources at the district scale requires proactive planning at both the facility and operational levels to ensure that each healthcare institution's strengths support the operational, infrastructure and thought leadership of the whole district.
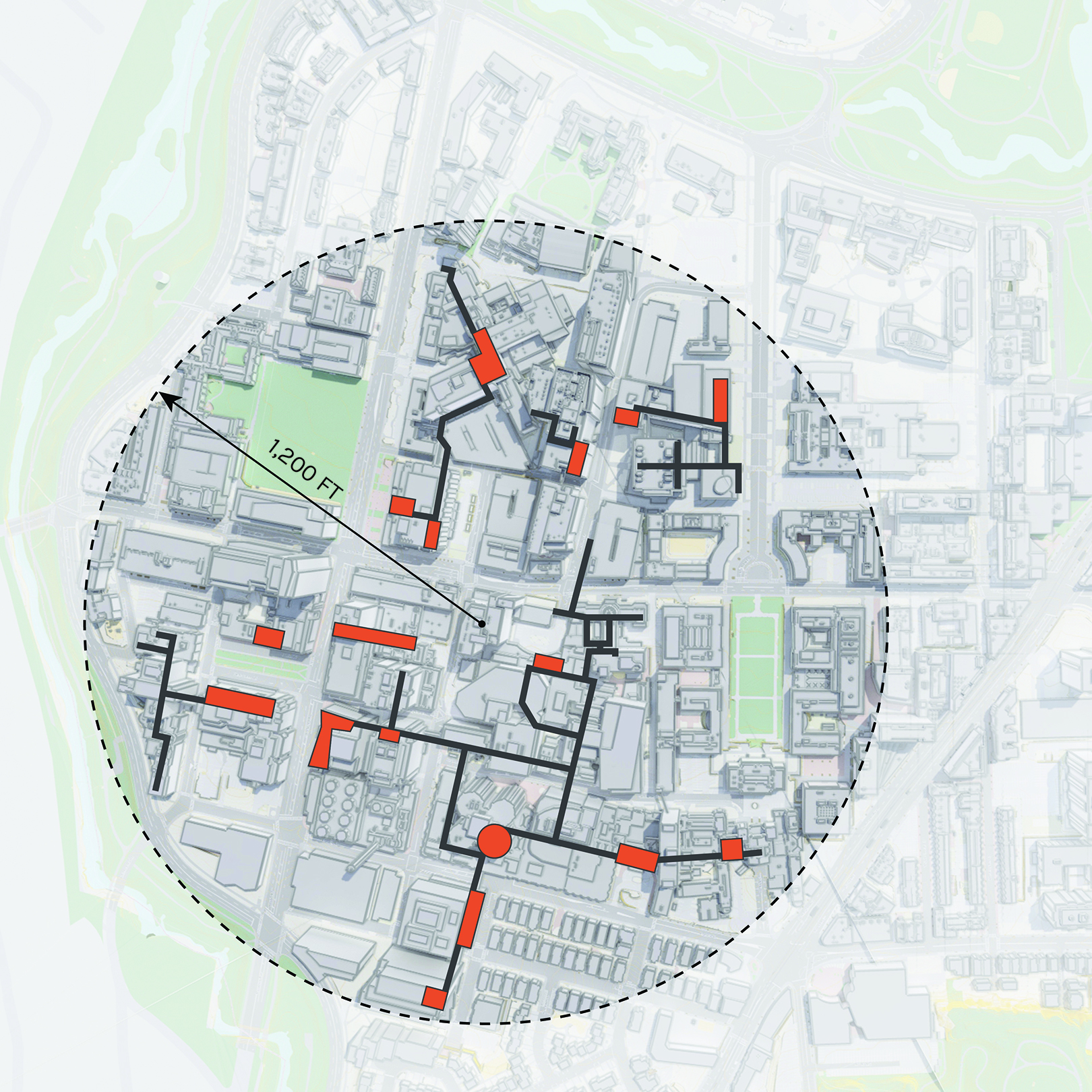 Lobbies and public circulation enable seamless connection between the five academic medical institutions in the dense urban Longwood Medical District. Combined they comprise an “interior public realm” as significant as the exterior open spaces in the district.
Lobbies and public circulation enable seamless connection between the five academic medical institutions in the dense urban Longwood Medical District. Combined they comprise an “interior public realm” as significant as the exterior open spaces in the district.
A key objective in optimizing medical district resources during a pandemic is the ability to expand, combine and reallocate medical resources (beds, ORs, exam rooms) while maintaining access to logistics infrastructure designed to support them. Licensed beds (ICU and med/surg) would be reserved for acute care patients (both pandemic and non-pandemic related). Existing treatment spaces like exam rooms and perioperative bays, with existing medical infrastructure (headwalls with medical gases, emergency electrical and nurse call), can be converted to alternative-use beds in planned stages to meet surging need. Proximal access to these combined resources and infrastructure would allow the use of pop-up hospitals in other civic locations, such as convention centers or arenas, for sub- or non-acute patients not requiring the same systems or environmental infrastructure.
Other resources are available in a typical medical district beyond clinical space. University residence halls can provide temporary housing for hospital staff and relief workers. These beds can also potentially support observation and sub-acute patients, freeing up hospital spaces for more acute cases. During the pandemic, a new high-rise residence hall at Emmanuel College, one of the LMA academic institutions, is housing staff from an adjacent medical center, including a dedicated floor for COVID-positive staff. Classroom and conference space can be used for emergency management and communications purposes. Research facilities within the district can provide crucial testing capacity and assist in developing targeted therapeutics and clinical trials. At the start of the 2019 pandemic, Vanderbilt UMC and other providers set-up triage and beds in an adjacent parking garage, directing incoming patient flow away from the emergency department.
The challenges in creating a district-wide plan abound. During a crisis event, institutions will need to prioritize the temporary integration of some operations of multiple institutions, competing cost structures, the need for central point of control, and wayfinding and access. Also, needs will differ dramatically in emergency events: a pandemic response may hinge on separation and isolation, whereas a mass casualty event centers on trauma services. Advanced planning and a standing emergency operating agreement between cooperating institutions would address issues such as leadership, governance, staff sharing, communications and liability.
The results of a well-developed, well-executed plan during a crisis would prove invaluable in saving lives and shortening response durations. The community benefits would include a greater breadth and flexibility of resources, increased scale of capacity, access to transit, and perhaps most compelling, access to an innovation mindset and the promise of novel treatment strategies and therapeutics.
Urban Planning Considerations for Medical District Preparedness
New medical districts are evolving as municipalities, private industry and academic medical centers aggregate into urban centers for health sciences innovation and entrepreneurship. Existing academic medical centers, many in urban environments, face unrelenting pressures to grow and modernize.
This natural evolution of capital development is an opportunity to incorporate partnerships and planning considerations that ensure resiliency. As medical districts evolve and academic medical centers grow and modernize, the following planning considerations share a district approach that enhances inter-institutional collaboration and scalability while preserving each institution's identity, branding and presence.
Circulation & Connectivity. Systems of sidewalks, roadways and public spaces should provide clear wayfinding, safety and capacity for pedestrians, bikes, transit, and passenger and service vehicles. In many existing academic medical centers, major public corridor systems span to connect multiple adjacent institutions. Public spaces placed at the intersection of institutions promote interaction, orientation, collaboration and district cohesion—and, in an emergency, important opportunities for information dissemination.
The Skyway at Cleveland Clinic and the Pike at Brigham and Women's Hospital were originally designed as primary circulation systems that connect key destinations. Decades later, major building expansion projects continue to expand these circulators to promote access, integration and connectivity.
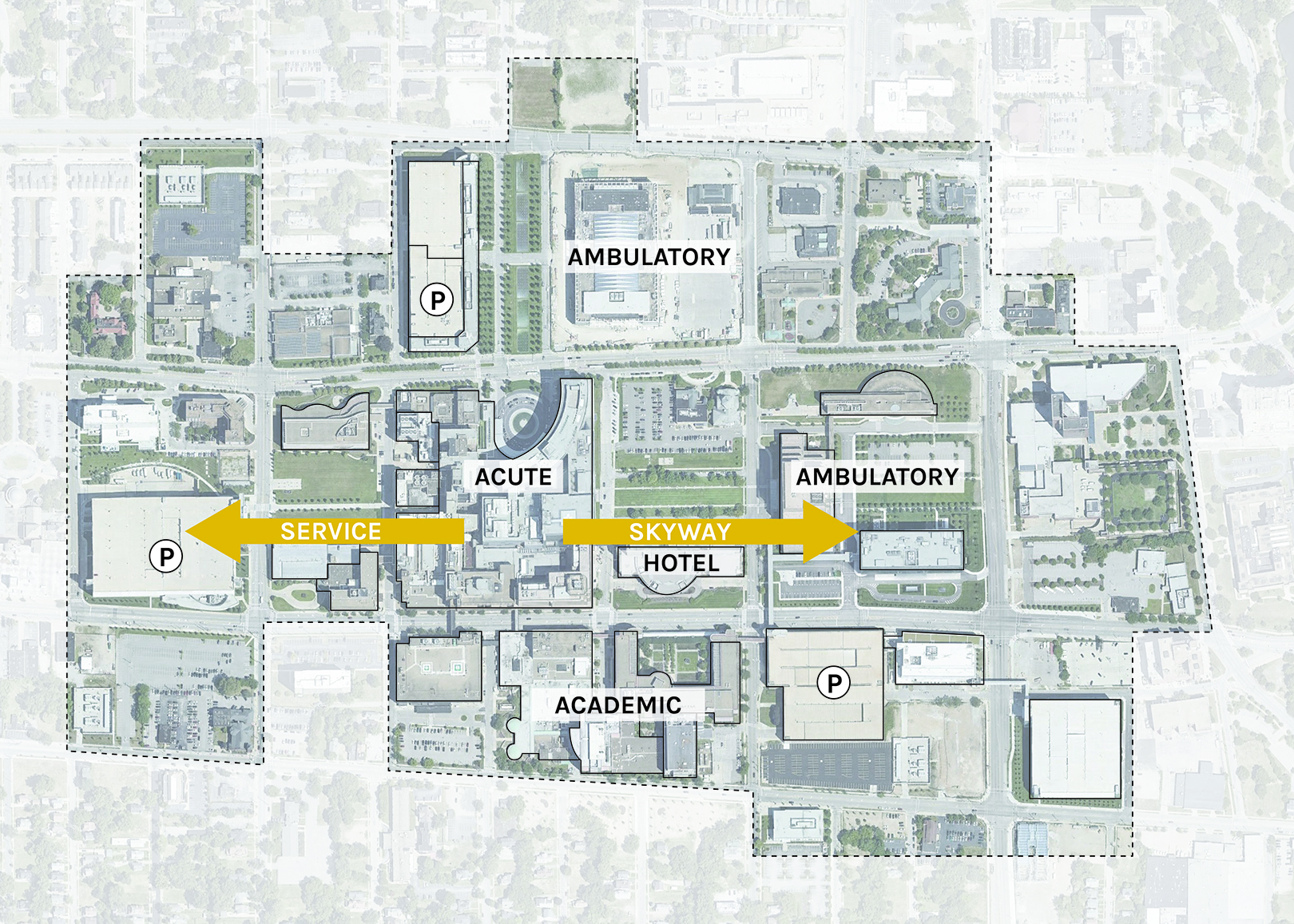 A dedicated parking and service facility connects via tunnel to the main acute complex at Cleveland Clinic, providing separation of service and pedestrian circulation. Similarly, the Skyway connects the outpatient and inpatient building complexes with the Intercontinental Hotel.
A dedicated parking and service facility connects via tunnel to the main acute complex at Cleveland Clinic, providing separation of service and pedestrian circulation. Similarly, the Skyway connects the outpatient and inpatient building complexes with the Intercontinental Hotel.
As institutions grow, opportunities to centralize service and materials distribution facilities may provide operational efficiencies, space savings, and improve inter-institutional flexibility in the event institutions need to work together in an emergency response. Design appropriately, public circulators could include the ability to move people as well as materials, allowing supplies, trash, linens and food to be more easily distributed across connected buildings—and institutions—in the event vehicular circulation or access to service docks is temporary disrupted or restricted.
Infrastructure. Medical districts are frequently aggregations of existing institutions that have evolved over time to share central utilities at some level: typically steam distribution, chilled water and power. This has resulted in resiliency vulnerabilities, such as below-grade utility tunnels at risk of flooding or chilled water piping approaching the end of useful life (which are extremely expensive and disruptive to service).
Modernization offers alternatives to the expensive replacement of buried infrastructure, often located below critical circulation roads and increasingly at-risk during water-related shocks and events. Microgrid strategies can provide district-wide redundancy and back-up while reducing dependency on extensive networks of buried infrastructure. At the district level, infrastructure can be shared as part of building connectors that also move people and materials. At the building level, infrastructure modernization should provide flexibility for air movement in infectious events, resiliency from flooding, and power self-sufficiency.
Communications infrastructure should allow robust connectivity between institutions and local emergency services, ensuring sustainable access to electronic medical records and responsive resource allocation such as patient transport, testing and PPE.
Access to Services. In cases where medical resources are aggregated across district institutions, access and wayfinding may be seen through a different lens. In an emergency event, a district approach enables each institution's departmental resources to be redistributed to meet the needs of the crisis; for example, each emergency department designated to receive exclusive case types or specific bed types and services delegated by hospital or bed tower. Ambulatory buildings or even an academic student center could function as the patient "front door" to other medical resources in the district. This would provide assessment, information and controlled access for the public and patients.
Mobility & Public Realm. Urban medical districts and academic medical center campuses must be planned to efficiently accommodate daily surges of students, patients and families, physicians, researchers, administrators and staff. In the Boston LMA, 112,000 people commute to and visit the 213-acre district daily. Like many of these districts, it benefits from convenient access to multiple transportation modes, including shuttles and city transit. It has also embraced Complete Streets principles such as bike and bus lanes, information kiosks, plantings and livable sidewalks. Initiatives such as these engage private industry and government to enhance safety, capacity and experience to support a diverse population of users under a range of operating conditions; which may, unfortunately, also include emergency events.
 Investment in circulation and social space can accommodate surges in user populations and provide opportunities for information dissemination and respite, all important during an emergency condition. The High Line in New York City connects buildings, institutions and adjacent districts. (Image by David Berkowitz from New York, NY, USA, used under Creative Commons license CC BY 2.0)
Investment in circulation and social space can accommodate surges in user populations and provide opportunities for information dissemination and respite, all important during an emergency condition. The High Line in New York City connects buildings, institutions and adjacent districts. (Image by David Berkowitz from New York, NY, USA, used under Creative Commons license CC BY 2.0)
The need to train interdisciplinary care teams to deliver better, more cost-effective healthcare has driven strategic, facility and district planning in academic medical centers and medical districts over the last two decades. Climate change and its resulting risks challenge the viability of existing real estate. In addition, the march of technology, evolving clinical service delivery models, facility obsolescence, increasing demand for trained medical professionals, and the practical need to commercialize discovery are all driving transformation in the institutions and districts that provide these services.
Add to this list the need for resilience to disruption. While many had predicted a potential pandemic, the current COVID-19 pandemic has dramatically increased the plausibility of similar crisis events in the future. As an evolving, dynamic urban ecosystem, the medical district is in a unique position to respond. The magic of planning—the opportunity to anticipate and accommodate change—is a critical strategic tool to meet these challenges.
More from Author

SmithGroup | Oct 28, 2024
A case for mid-rise: How multifamily housing can reshape our cities
Often referred to as “five-over-ones,” the mid-rise apartment type is typically comprised of five stories of apartments on top of a concrete “podium” of ground-floor retail. The main criticism of the “five-over-one” is that they are often too predictable.

SmithGroup | Mar 28, 2023
Inclusive design requires relearning how we read space
Pulling from his experience during a campus design workshop, David Johnson, AIA, LEED AP, encourages architects to better understand how to design spaces that are inclusive for everyone.

SmithGroup | Feb 27, 2023
Surfing the Metaversity: The future of online learning?
SmithGroup's tour of the Metaversity gives us insight on bringing together physical and virtual campuses to create a cohesive institution.

SmithGroup | Nov 28, 2022
Data centers are a hot market—don't waste the heat!
SmithGroup's Brian Rener shares a few ways to integrate data centers in mixed-use sites, utilizing waste heat to optimize the energy demands of the buildings.

SmithGroup | Aug 3, 2022
Designing learning environments to support the future of equitable health care
While the shortage of rural health care practitioners was a concern before the COVID-19 pandemic, the public health crisis has highlighted the importance of health equity in the United States and the desperate need for practitioners help meet the needs of patients in vulnerable rural communities.

SmithGroup | Aug 10, 2021
Retail reset: The future of shopping malls
Developers and design partners are coming together to reimagine how malls can create a new generation of mixed-use opportunities.

SmithGroup | Jan 25, 2021
Amid pandemic, college students value on-campus experience
All the students we interviewed were glad that they returned to campus in one form or another.

SmithGroup | Aug 13, 2020
Renewing the healing role of public parks
While we can’t accurately predict all the ways we will respond to the current COVID-19 pandemic, it should provide a moment of reflection as we see all too clearly the consequences of our exploitation and destruction of nature.

SmithGroup | Jul 21, 2020
How design of senior living communities must change after COVID-19
The cost of maintaining high quality of care and high quality of life for senior living communities has increased up to 73% for senior living communities that remain free of COVID-19 and up to 103% for COVID-19 positive senior living communities.

SmithGroup | Jun 12, 2020
How will museums change after COVID-19
This new environment may herald innovative economic models and change the way we think about museum design.



