

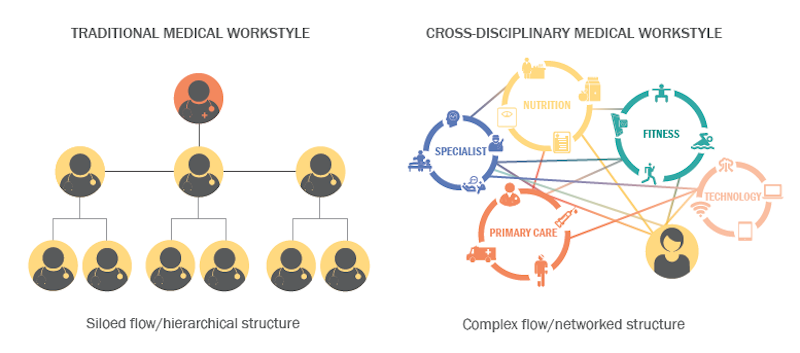
“Collaboration” has become an abiding design goal for many nonresidential building types, such as offices and educational institutions. But the medical field, with its hierarchical divisions and silo mentality among professionals, continues to resist a more collaborative workplace culture.
Perkins Eastman set out to find out why, and used one of its own projects—the 95,000-sf NYU Winthrop Hospital Research and Academic Center in Mineola, N.Y.—as a test case a year after it opened in 2015.
The firm's post-occupancy evaluation—whose findings it published in a recently released white paper “The Effectiveness of Collaborative Spaces in Healthcare and Research Environments”—focuses on the activities within a third-floor multi-use space in the facility that the firm designed specifically with employee interaction in mind.
The white paper touches on the evolution of collaborative design, and singles out two examples—Bell Labs’ headquarters in Murray Hill, N.J., in the 1960s, and Google’s national headquarters in Mountain View, Calif.—where cross-disciplinary collaboration took root and where “activity based” working is now on full display.
The paper notes that offices and education facilities are creating these kinds of environments by planning for collaboration early in the design process, “to include a variety of different kinds of areas to support one-on-one, individual, small group and large groupings.”
However, even the most thoughtfully designed space won’t lead to meaningful change in a workspace if it isn’t supported by policies and attitudes that foster collaboration. And that support is what Perkins Eastman found was missing at NYU Winthrop Research and Academic Center.
Its third-floor space was seen as a microcosm of Perkins Eastman’s design intent. Its programmatic elements include a pantry with small cook and prep area and two vending machines, a café dining space with tables and chairs, a break area with soft seating, a low four-person conference table and sit-up bar; a work room with a TV, tablet chairs and writable magnetic wall; a research area with a large writable wall, movable ottomans, and high-top tables and writing table tops; and a conference room with a large executive meeting table, digital projection capabilities, wet bar and seating banquette.
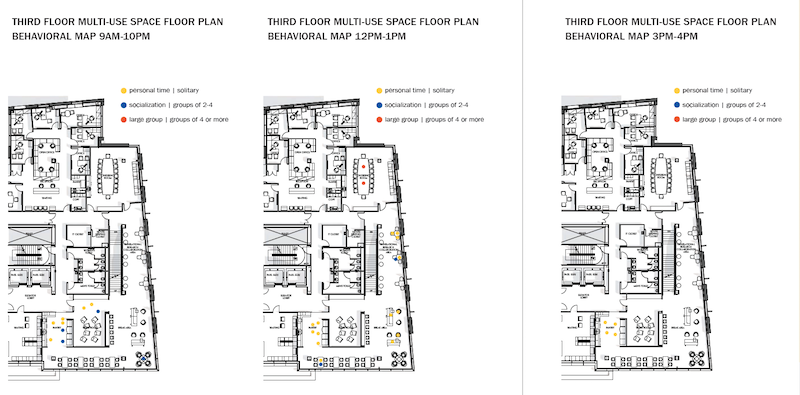
To assess employee engagement in a multi-use space within NYU Winthrop's Research and Academic Center, Perkins Eastman observed and place-mapped activities over a nine-hour period in several time intervals. It found scant indepartmental connectivity, and virtually no use of this space for work. Image: Perkins Eastman
Perkins Eastman observed and place-mapped employee interactions in that space over a nine-hour period in four intervals during the day. The firm tracked how long people spent in any one place, and what they were doing. It also noted whether people were alone or in groups.
“Very little interaction among users from different departments was observed,” Perkins Eastman found. Most people used to space to eat their lunches or talk on their phones. And they usually hung out with people from their own departments. “No spontaneous meetings of small or large groups were observed, and the amenities provided to support impromptu collaboration…went unused.”
Subsequent interviews with 17 user groups from various departments found that while employees generally like the space, they didn’t know how to use it other than to eat lunch or buy food from the vending machines.
None of the people interviewed used the space for work, primarily because their jobs require computers and other tools located at their designated workstations. More surprising, though, was the finding that many of the interviewees weren’t sure if they were even allowed to use the third-floor space for meetings or presentations. In fact, they were “simply uninformed about the potential uses of the third-floor space,” the white paper reports.
Perkins Eastman found that most doctors, researchers, nurses, and administrators within the user groups interviewed would like to collaborate. But a suggestive design wasn’t enough to instigate that interaction. “The faculty and staff needed to be shown how to use the third-floor in order to promote its use as a collaborative space.”
The white paper concedes that research often requires quiet, focused study supported by specialized workstations or lab equipment. And the need for privacy can be a barrier to collaborating in a healthcare environment.
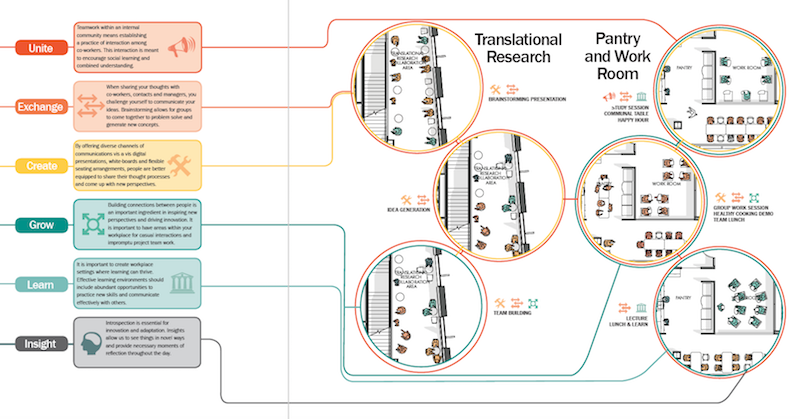
The white paper provides ways that medical centers could encourage collaborative use of their common spaces. The suggestions revolve around providing workers with more imformation about the potential uses of those areas. Image: Perkins Eastman
But there are “simple measures” that the Center could do to foment collaboration and communication, at least in the multi-use space with an open floor plan. These include:
•Create a schedule of programs and presentations for that space
•Assign an IT specialist to educate and assist users with technologies provided in the workroom and conference room
•Post information and signage that suggests how the space can be used
•Orient new employees about how to use the space, and
•Provide greater spatial variety, and the ability to close certain spaces for private meetings. (A number of interviewees said they didn’t conduct meetings on the third floor because none of the rooms could be closed off.)
In the final analysis, Perkins Eastman remains convinced that design, reinforced by programming, can support collaboration and employee engagement within a medical building. But the medical profession also needs to shift toward a more positive attitude about collaboration. “If users are uninformed about the potential uses of a space, it is difficult for a culture of collaboration to thrive.”
Related Stories

| Dec 29, 2014
New mobile unit takes the worry out of equipment sterilization during healthcare construction [BD+C's 2014 Great Solutions Report]
Infection control, a constant worry for hospital administrators and clinical staffs, is heightened when the hospital is undergoing a major construction project. Mobile Sterilization Solutions, a mobile sterile-processing department, is designed to simplify the task. The technology was named a 2014 Great Solution by the editors of Building Design+Construction.

| Dec 29, 2014
HealthSpot station merges personalized healthcare with videoconferencing [BD+C's 2014 Great Solutions Report]
The HealthSpot station is an 8x5-foot, ADA-compliant mobile kiosk that lets patients access a network of board-certified physicians through interactive videoconferencing and medical devices. It was named a 2014 Great Solution by the editors of Building Design+Construction.

BIM and Information Technology | Dec 28, 2014
The Big Data revolution: How data-driven design is transforming project planning
There are literally hundreds of applications for deep analytics in planning and design projects, not to mention the many benefits for construction teams, building owners, and facility managers. We profile some early successful applications.
 Campus, the Building Team took advantage of the sites natural coastal g")
| Dec 28, 2014
AIA course: Enhancing interior comfort while improving overall building efficacy
Providing more comfortable conditions to building occupants has become a top priority in today’s interior designs. This course is worth 1.0 AIA LU/HSW.

| Dec 2, 2014
Nonresidential construction spending rebounds in October
This month's increase in nonresidential construction spending is far more consistent with the anecdotal information floating around the industry, says ABC's Chief Economist Anirban Basu.

| Dec 1, 2014
How public-private partnerships can help with public building projects
Minimizing lifecycle costs and transferring risk to the private sector are among the benefits to applying the P3 project delivery model on public building projects, according to experts from Skanska USA.

| Nov 25, 2014
Emerging design and operation strategies for the ambulatory team in transition
As healthcare systems shift their care models to be more responsive to patient-centered care, ambulatory care teams need to be positioned to operate efficiently in their everyday work environments, write CannonDesign Health Practice leaders Tonia Burnette and Mike Pukszta.

| Nov 20, 2014
Lean Led Design: How Building Teams can cut costs, reduce waste in healthcare construction projects
Healthcare organizations are under extreme pressure to reduce costs, writes CBRE Healthcare's Lora Schwartz. Tools like Lean Led Design are helping them cope.

| Nov 18, 2014
5 big trends changing the world of academic medicine
Things are changing in healthcare. Within academic medicine alone, there is a global shortage of healthcare professionals, a changing policy landscape within the U..S., and new view and techniques in both pedagogy and practice, writes Perkins+Will’s Pat Bosch.

| Nov 14, 2014
Haskell acquires FreemanWhite, strengthens healthcare design-build business
The combination expands Haskell’s geographic presence by adding FreemanWhite’s offices in Chicago, Charlotte, Nashville, and San Diego. FreemanWhite will retain its name and brand.



