

Georgia Tech’s SimTigrate Design Lab and Dräger, an international supplier of medical and safety technology, have released a white paper that sets out to demonstrate the advantages for Intensive Care Units in hospitals of ceiling-mounted beam systems over traditional headwall systems or those operated with articulated arms or overhead booms.
One of this paper’s stated purposes is to understand how medical teams evaluate architectural solutions to medical gas delivery, and to compare user experiences with different overhead utilities in the ICU. Its opinions are based primarily on field observations of the use of booms in three hospitals, interviews with staff in other ICUs who have used the beam system, and a simulation conducted in a low-fidelity mockup with nurses, physicians and respiratory therapists from a hospital undergoing a renovation of its ICU patient rooms.
The paper is also a full-throated endorsement of Dräger’s beam system for ICUs, although it does not delve into cost comparisons among different delivery systems.
The paper observes that operating rooms in most hospitals already favor ceiling-mounted systems to deliver medical gases and supply power. As more patient care is provided at the bedside within ICUs, hospitals have replicated overhead service delivery solutions in those units to realize the same advantages of improved access to the head of the bed.
“Yet it is important to keep in mind that ICU rooms do not function exactly like operating rooms, and therefore may have different needs,” the paper states.
The white paper spells out the disadvantages of headwalls in ICUs (space, patient and equipment access, mobility). It also provides a number of reasons why overhead booms aren’t optimal, either.
For example, while overhead booms free up floor space, “they are quite large and take up a lot of real estate in the patient room.” Due to limited space in most inpatient rooms, nurses routinely have to move both boom arms out of the way to move patients into or out of the room.
The flexibility of articulated boom arms has a downside, too, in that the arms can block critical views of such things as monitors.
Perhaps the biggest disadvantage of booms operating overhead is that they impede the use of patient lifts, because the range of a cross bar is limited by the boom and requires that the boom arms are pushed all the way forward, and the bed be moved further away from the wall, to gain access to the patient’s center of gravity.
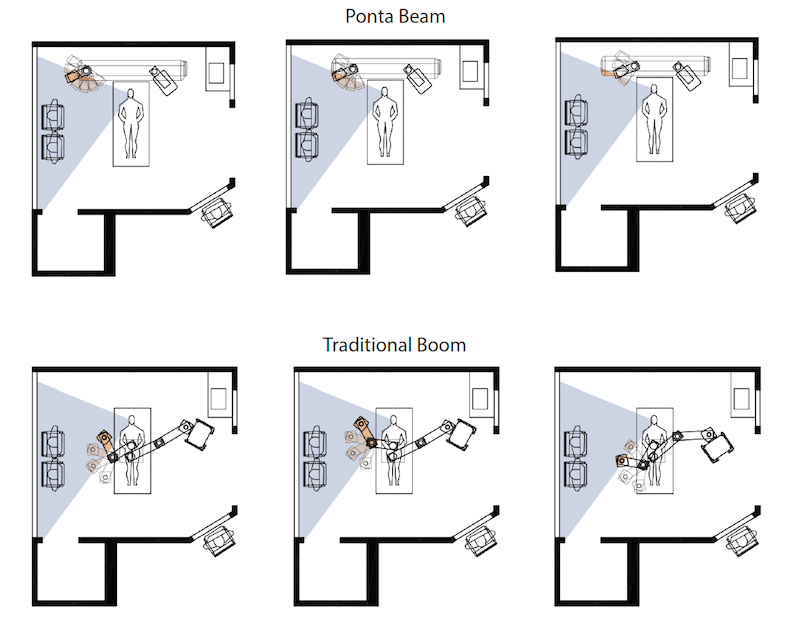
These illustrations compare patient access when an ICU room is equipped with a Ponta beam system (top) versus an articulated arm system. The Georgia Tech white paper says the biggest disadvantage of booms operating overhead or to the side of the bed is that they impede the use of patient lifts, because the range of a cross bar is limited by the boom and requires that the boom arms are pushed all the way forward, and the bed be moved further away from the wall, to gain access to the patient’s center of gravity. Image: “Comparison of Overhead Utility Systems for Intensive Care Rooms.”
The bulk of this white paper is devoted to demonstrating the advantages of Dräger’s Ponta overhead beam system within an ICU environment.
It states that the Ponta beam takes up less space than an overhead boom, which is important for smaller inpatient rooms. The beam system allows nurses to move the shuttles (columns that suspend from the beam) laterally to come closer together to support infants in incubators or patients in chairs; or farther apart to support bariatric patients.
The columns are customizable for the specific needs of the ICU clinic and standardized across all rooms, such that the ventilator is always on the same side of the patient bed. The beam system allows staff to move the bed in and out of the room easier.
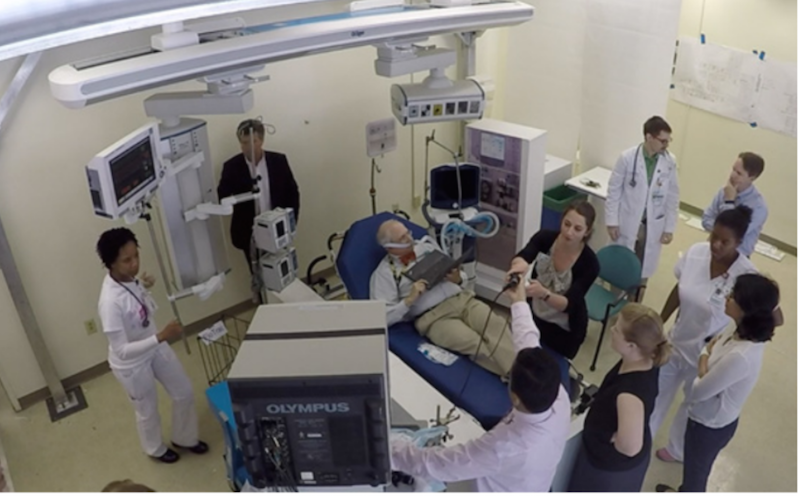
To back up its claims, Georgia Tech, with support from Dräger, the architectural firm HKS, and Grady Health System, conducted three simulation sessions on the Grady’s campus in downtown Atlanta to give the nurses, providers, and facility leadership an opportunity to try out the Ponta beam under real-life care situations.
A critical care doctor with Grady scripted a complex patient scenario that required bulky equipment, access to the head of the bed, and placed many people in the room.
The participants included nurses, doctors, and leadership from Grady’s medical ICU, as well as nurses from the Marcus Stroke and Neurosciences Center who were familiar with using a boom and could compare the performance of different delivery systems.
The 15 simulation participants who completed surveys rated the Ponta system positively in all categories. A dozen agreed or strongly agreed that the beam reduced clutter around the bed; 13 agreed or strongly agreed that the beam better organizes equipment, and 11 agreed or strongly agreed that the beam system is better for managing cables.
Clear majorities of participants also judged the beam system superior to overhead boom systems for providing better access to the patient and to gases and equipment, and better visibility to monitors.
“It is clear that ceiling-mounted solutions for delivery of utilities are far superior than the traditional headwall,” the report states. But unlike overhead boom systems, which were designed originally for operating rooms, Dräger’s Ponta beam system is specifically desgined for smaller inpatient room. The beam system also minimizes bulky infrastructure directly over the patient.
Perhaps the biggest advantage of the Ponta beam is that because it is not mounted directly over the center of the bed, that space is available for overhead patient lift tracks, making the patient lift more effective and easier to operate, which results in more frequent use.
Related Stories
| Aug 11, 2010
Stimulus funding helps get NOAA project off the ground
The award-winning design for the National Oceanic and Atmospheric Administration’s new Southwest Fisheries Science Center replacement laboratory saw its first sign of movement last month with a groundbreaking ceremony held in La Jolla, Calif. The $102 million project is funded primarily by the American Recovery and Reinvestment Act.
| Aug 11, 2010
National Intrepid Center tops out at Walter Reed
SmithGroup, Turner Construction, and the Intrepid Fallen Heroes Fund (IFHF), a nonprofit organization supporting the men and women of the United States Armed Forces and their families, celebrated the overall structural completion of the National Intrepid Center of Excellence (NICoE), an advanced facility dedicated to research, diagnosis, and treatment of military personnel and veterans sufferin...
| Aug 11, 2010
Alabama hospital gets a four-story addition
Birmingham, Ala.-based Hoar Construction has completed the North Tower addition at Thomas Hospital in Fairhope, Ala. The four-story, 123,000-sf addition accommodates an ER on the first floor, 32 private patient rooms and nursing support on the second and third floors, and room for 32 planned patient rooms on the top floor.
| Aug 11, 2010
America's Greenest Hospital
Hospitals are energy gluttons. With 24/7/365 operating schedules and stringent requirements for air quality in ORs and other clinical areas, an acute-care hospital will gobble up about twice the energy per square foot of, say, a commercial office building. It is an achievement worth noting, therefore, when a major hospital achieves LEED Platinum status, especially when that hospital attains 14 ...
| Aug 11, 2010
Hospital Additions + Renovations: 14 Lessons from Expert Building Teams
Two additions to a community hospital in Ohio that will double its square footage. A 12-story addition on top of an existing 12-story tower at Houston's M.D. Anderson Cancer Center. A $54 million renovation and addition at the University of Virginia Medical Center. A 67-bed, $70 million addition/renovation to a community hospital that is only five years old.
| Aug 11, 2010
Research Facility Breaks the Mold
In the market for state-of-the-art biomedical research space in Boston's Longwood Medical Area? Good news: there are still two floors available in the Center for Life Science | Boston, a multi-tenant, speculative high-rise research building designed by Tsoi/Kobus & Associates, Boston, and developed by Lyme Properties, Hanover, N.
| Aug 11, 2010
3 Hospitals, 3 Building Teams, 1 Mission: Optimum Sustainability
It's big news in any city when a new billion-dollar hospital is announced. Imagine what it must be like to have not one, not two, but three such blockbusters in the works, each of them tracking LEED-NC Gold certification from the U.S. Green Building Council. That's the case in San Francisco, where three new billion-dollar-plus healthcare facilities are in various stages of design and constructi...
| Aug 11, 2010
Holyoke Health Center
The team behind the new Holyoke (Mass.) Health Center was aiming for more than the renovation of a single building—they were hoping to revive an entire community. Holyoke's central business district was built in the 19th century as part of a planned industrial town, but over the years it had fallen into disrepair.
| Aug 11, 2010
Right-Sizing Healthcare
Over the past 30 years or so, the healthcare industry has quietly super-sized its healthcare facilities. Since 1980, ORs have bulked up in size by 53%, acute-care patient rooms by 77%. The slow creep went unlabeled until recently, when consultant H. Scot Latimer applied the super-sizing moniker to hospitals, inpatient rooms, operating rooms, and other treatment and administrative spaces.
| Aug 11, 2010
Great Solutions: Healthcare
11. Operating Room-Integrated MRI will Help Neurosurgeons Get it Right the First Time A major limitation of traditional brain cancer surgery is the lack of scanning capability in the operating room. Neurosurgeons do their best to visually identify and remove the cancerous tissue, but only an MRI scan will confirm if the operation was a complete success or not.



