


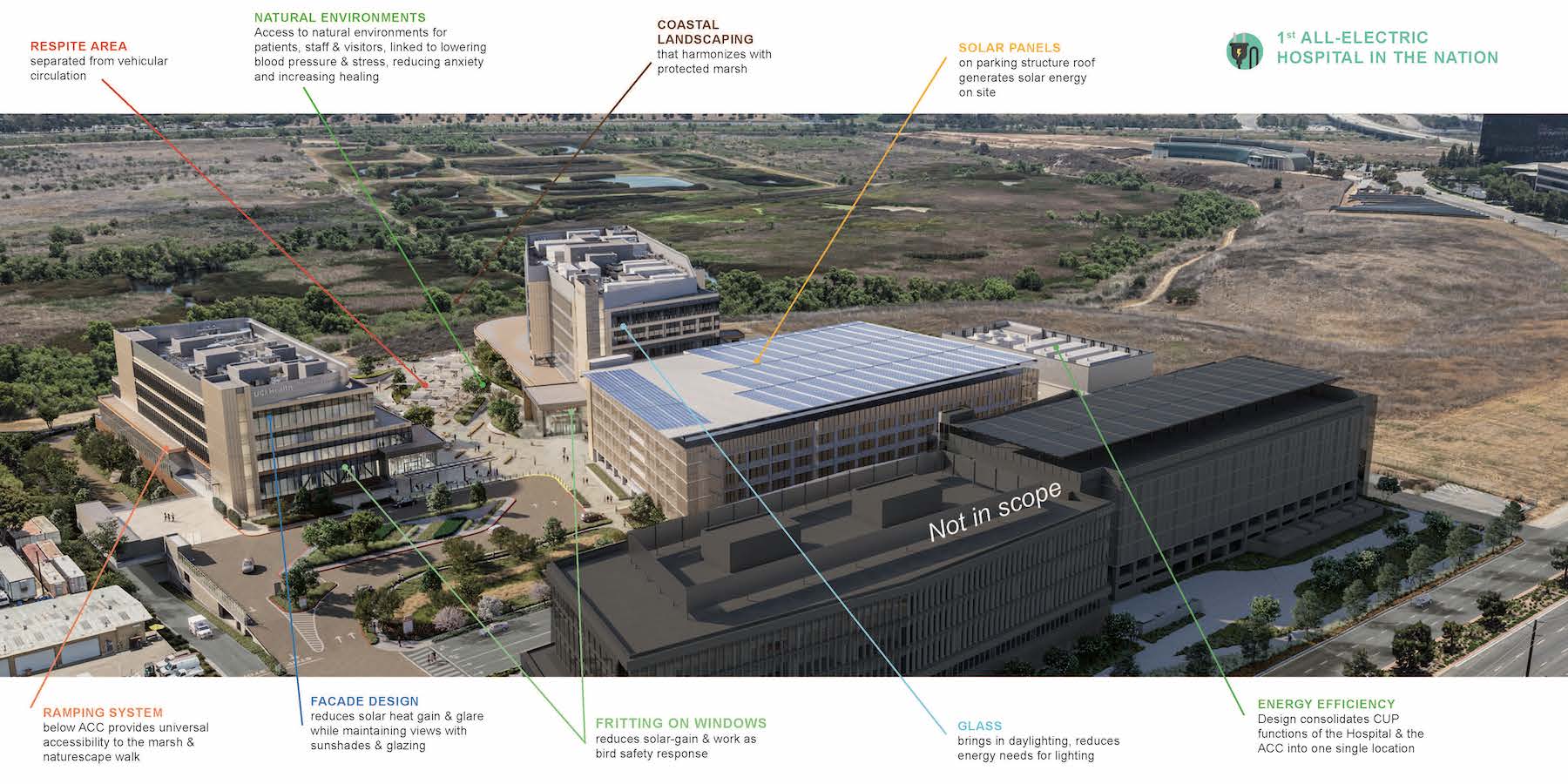
The University of California at Irvine (UCI) has a track record for sustainability. It recently received LEED Platinum certification for its 23rd campus building. Its under-construction UCI Medical Center is designed, positioned, and built to preserve the nearby San Joaquin Marsh Reserve, to reduce the facility’s solar gain by 85%, and to be the first medical center in the country to operate on an all-electric central plant.
The University of California’s system favors sustainable solutions, including its requirement that new construction be all-electric. Instead of filing for a waiver, UCI determined that it could meet that requirement “at only a modest premium,” says Brian Pratt, UCI Campus Architect and Associate Vice Chancellor. (The premium would be around $2.5 million on a project whose construction cost is $770 million and all-in cost will be over $1 billion.)
UCI Medical Center will consist of a four-story, 357,000-sf hospital with 144 beds, operating rooms, 20 Emergency Department beds, and 16 acute observation beds; a 223,000-sf Comprehensive Cancer and Ambulatory Care Center with 36 exam rooms, outpatient surgery, labs, and a pharmacy; a 35,000-sf central plant; and a parking structure with 1,340 spaces.
The parking structure was completed last year, and the outpatient building and central plant are scheduled for completion next year. The hospital should be done in 2025. To meet California and national code requirements, the power system will be backed up by diesel fuel generators (see Editor's note below).

Electrification without compromise
The decision to go all-electric was made early in the design process, recalls Khristina Stone, Preconstruction Manager for the GC Hensel Phelps, which with CO Architects leads the Progressive Design-Build team on this project. Nick Spady, Hensel Phelps’ Operations Manager, says that installing the buildings’ electrical infrastructure and emergency generators pose the greatest challenges in an all-electric environment.
The bridging documents actually described an electric heating system that allowed for the use of natural gas for steam. But ultimately the design-build team and the university decided to dispense with steam boilers altogether, says Roger Carter, CEO and Senior Principal of tk1sc, the project’s MEP engineer.

Carter notes that state codes now require hospital rooms to have constant air volume, which can impact the heating system’s’ load. An all-electric system will allow UCI’s hospital to leverage the central plant’s heat-recovery chillers to manage the building’s energy performance. Indeed, going all-electric is not expected to compromise the medical center’s operations, whose universal design allows for all patient rooms to be converted to intensive care units.
UCI Medical Center is being built under a Progressive Design-Build contract, which Pratt says has been the university’s bid-out preference for decades. He notes that hospital projects are complicated with many stakeholders, and a Progressive Design-Build agreement “allows for expert feedback earlier in the project.”
He notes, parenthetically, that prior to construction UCI had worked with the architect HOK for a year on the medical center’s programming. “This put up guardrails on the project, but with enough room for flexibility.” Gina Chang, CO Architects’ Principal and Healthcare Team Lead, says there was also a program alignment period, during which the team could receive comment and suggestions from UCI and the hospital’s users.
“The bridging documents weren’t overly heavy, so the contract set up a more positive relationship [with UCI] for flexibility and creativity,” says Stone.
The rest of the Progressive Design-Build team includes Degenkolb (SE), Stantec (CE), Ridge Landscape Architects (LA), Newson Brown Acoustics (acoustical engineer), and Colin Gordon Associates (acoustical vibration).
Indoor and outdoor wellness
Aside from its electrification, UCI Medical Center features other sustainable elements. For example, the choice of brace framing, which Pratt says was “rooted in resilience,” reduces the project’s measurable embodied carbon by 20 percent. CO’s Chang further explains: “We implemented the lightest structural system possible (BRBF buckling restrained braced frame) to reduce the embodied carbon footprint. Though we sought for carbon reduction also with the concrete design, the site had high levels of methane and other greenhouse gasses that needed to be contained, so a larger, mat footing was utilized to mitigate that problem.”

After conducting several frit and shading studies, the design team optimized the building’s envelope to reduce its solar gain by 85 percent, and to minimize bird strikes.
The medical center will also tap into the city of Irvine’s robust recycled water infrastructure.
Chang says the marsh—which is managed by UCI biologists—drove the massing and position of the buildings. “We took seriously being a good neighbor to the marsh,” adds Pratt. The construction site includes a turtle fence. And the biologists said that runoff from the site was fine as long as it was treated.

Like most healthcare facilities, UCI Medical Center is placing a premium on wellness. It has multiple areas for gathering outdoors, including walkable pathways and so-called healing gardens that offer views of the landscaping. (The outside plaza between the hospital and outpatient buildings brushes up against the edge of the marsh.)
“The landscape design and plant palette matter,” says Pratt. “And the marsh in the differentiator.” Indoors are numerous terraces, and other places of respite that include “lavender” rooms where staff members under stress can retreat.
________
Editor's note: After this story was posted, Ray Swartz, an engineer and Senior Principal with tk1sc, the project's MEP engineer, responded to a reader's question about the Medical Center's backup power source in the event of an electrical outage:
Swartz said that California's Department of Health Care Access and Information enforces a minimum of 72 hours of fuel storage for a new NPC-5 building, not the 96 hours required by NFPA 110. However, NFPA 110 requires the main fuel tank(s) to have a minimum capacity of at least 133 percent of the quantity needed by CEC 700.12 (B) (2) Exception 1 or 2. Therefore, for NPC-5 buildings, the minimum capacity requirement is 133 percent of the 72-hour fuel supply, equating to 96 hours.
The UCI Medical Center project includes four 3,000-kW generators operating in parallel. The capacity is adequate to service the campus in a 100 percent business-as-usual format. The generators are diesel fuel type, and the campus has an underground fuel storage capacity of 65,000 gallons. If, in an emergency, refueling the tanks is feasible, the campus could operate continuously under generator power.
Related Stories

| Dec 29, 2014
New mobile unit takes the worry out of equipment sterilization during healthcare construction [BD+C's 2014 Great Solutions Report]
Infection control, a constant worry for hospital administrators and clinical staffs, is heightened when the hospital is undergoing a major construction project. Mobile Sterilization Solutions, a mobile sterile-processing department, is designed to simplify the task. The technology was named a 2014 Great Solution by the editors of Building Design+Construction.

| Dec 29, 2014
HealthSpot station merges personalized healthcare with videoconferencing [BD+C's 2014 Great Solutions Report]
The HealthSpot station is an 8x5-foot, ADA-compliant mobile kiosk that lets patients access a network of board-certified physicians through interactive videoconferencing and medical devices. It was named a 2014 Great Solution by the editors of Building Design+Construction.

BIM and Information Technology | Dec 28, 2014
The Big Data revolution: How data-driven design is transforming project planning
There are literally hundreds of applications for deep analytics in planning and design projects, not to mention the many benefits for construction teams, building owners, and facility managers. We profile some early successful applications.
 Campus, the Building Team took advantage of the sites natural coastal g")
| Dec 28, 2014
AIA course: Enhancing interior comfort while improving overall building efficacy
Providing more comfortable conditions to building occupants has become a top priority in today’s interior designs. This course is worth 1.0 AIA LU/HSW.

| Dec 2, 2014
Nonresidential construction spending rebounds in October
This month's increase in nonresidential construction spending is far more consistent with the anecdotal information floating around the industry, says ABC's Chief Economist Anirban Basu.

| Dec 1, 2014
How public-private partnerships can help with public building projects
Minimizing lifecycle costs and transferring risk to the private sector are among the benefits to applying the P3 project delivery model on public building projects, according to experts from Skanska USA.

| Nov 25, 2014
Emerging design and operation strategies for the ambulatory team in transition
As healthcare systems shift their care models to be more responsive to patient-centered care, ambulatory care teams need to be positioned to operate efficiently in their everyday work environments, write CannonDesign Health Practice leaders Tonia Burnette and Mike Pukszta.

| Nov 20, 2014
Lean Led Design: How Building Teams can cut costs, reduce waste in healthcare construction projects
Healthcare organizations are under extreme pressure to reduce costs, writes CBRE Healthcare's Lora Schwartz. Tools like Lean Led Design are helping them cope.

| Nov 18, 2014
5 big trends changing the world of academic medicine
Things are changing in healthcare. Within academic medicine alone, there is a global shortage of healthcare professionals, a changing policy landscape within the U..S., and new view and techniques in both pedagogy and practice, writes Perkins+Will’s Pat Bosch.

| Nov 14, 2014
Haskell acquires FreemanWhite, strengthens healthcare design-build business
The combination expands Haskell’s geographic presence by adding FreemanWhite’s offices in Chicago, Charlotte, Nashville, and San Diego. FreemanWhite will retain its name and brand.



